
Resolution WHA56.19
Prevention and control of influenza pandemics and annual epidemics

‘… many of these deaths could be prevented through increased use particularly in people at high risk, of existing vaccines, which are safe and highly effective…‘
-
It’s the WHA56.19 resolution from May 28, 2003, probably the earliest express call for a 'model plan' (ie, a pandemic treaty).

-
The pro-vaccine quote above is hammered home repeatedly. In fact, if there’s one thing you can be certain of, it’s that vaccine manufacturers would still exist, should a pandemic kill 99% of the global population. Who else would protect us?
In fact, in bullet form, what the document states is that vaccines -
Can prevent influenza deaths - even ‘existing’ ones.
Should be timely manufactured.
The lack of vaccines (initially surveillance) causes economic hardship.
Said hardship isn’t actually documented, so should be investigated in nations with no recorded influenza problem.
Are safe and highly effective.
Require more manufacturing capacity.
Should see better use during epidemics.
Coverage in nations with existing vaccination plans should reach 50% by 2006, and 75% by 2010 in people deemed of high risk.
In nations without a such plan, the economic impact of influenza should be assessed, and this used to sell vaccines and install surveillance through public policy.
The need for adequate supplies during pandemic must be ensured.
R&D should be publicly supported to find the utopian vaccine which once and for all will cure influenza.
Member states should estimate required vaccine supplies to cope with potential pandemic.
Equitable access should be granted, ie, vaccines for all.
To accomodate this, public-private-partnerships are required.
Did you get all that? Good. Before addressing these, let’s also round up what else the WHO deman-… requests per this resolution.
Early detection.
Detection means surveillance.
We also need pandemic plans. National and global.
Disease surveillance is paramount in regards to these plans.
The WHO is doing a splendid job, according to the WHO.
The WHO needs to engage with, well, everyone but the public. Especially NGOs and private interests.
The WHO should provide leadership in the regard of all things pandemic.
In short - the WHO state that they should pen a pandemic plan to be implemented globally, ultimately be in charge in the event of a pandemic (which they get to call), that surveillance needs rolling out globally to detect for a potential pandemic, and national governments should ensure ‘adequate’ supplies of vaccines, when… sorry, if a pandemic strikes.
Or even shorter - the WHO will call a pandemic on basis of global surveillance data, and to get out of said pandemic state, you will have to take your vaccine.
Don’t you feel protected already?
And more on the ‘Global agenda on influenza surveillance and control‘ in a minute, which details the global surveillance they have in mind. But first - vaccines.
-
To sum up the points above more clearly, here they are again -
Manufacturing capacity is required
Stockpiles of vaccines in advance are required
Vaccine uptake should be increased
R&D efforts should be stepped up
Public-private-partnerships
Manufacturing capacity would clearly benefit the companies producing said vaccines, ie big pharma. This point alone spans two above - the demand for more capacity, and their timely manufacture, though the latter also bridges the next bullet point; stockpiles.
Stockpiles really is somewhat of an odd one in the context of influenza and other rapidly mutating virus infections - old vaccines do - at best - literally nothing given the contemporary strain having moved on. But it does act like another giant financial gain for big pharma. In addition to the half point above this also captures two bullet points above; need for adequate supplies, and vaccine supply estimates.
Uptake is another massive win for big pharma. More customers. Three points above are dedicated here; better use means more people should take the vaccine, the coverage percentages are higher than present figures, leading to higher uptake, and the equitable access ensures that even those who can’t afford to pay for said vaccines will receive, as they’re paid for by those who can.
R&D relates to big pharma demanding public money be used to subsidise the research and development stages of producing the vaccines. Now, this is typically the most expensive part of vaccine development, so yet again, a massive bonus for big pharma.
Finally, the request for public-private-partnership involvement will inevitably lead to private influence over the already heavily captured WHO - typically by big pharma lobby organisation - oh wait, here’s one.
The ESWI

The ESWI was officially founded in 1993 at the Pasteur Institute in Paris. Prior to formation, the first official meet took place at the ‘Options for the Control of Influenza II' in Courchevel, September, 1992. Kind of telling, really - Courchevel is
In other words, WHA56.19 might just as well have been penned by big pharma itself. In fact, given other involvement by the ESWI, it probably was.
-
On the matter of surveillance, the Global Agenda on Influenza was released in 2002. This document similarly is a crime scene, although a different one.
First off, this is to protect people, and vaccine messaging also exists throughout. But we already saw that component in the WHA above, consequently, I wish to set it aside as it doesn’t really contribute anything new.
Instead, what this document serves in terms of requests -
Influenza surveillance control
Prevention, control, and preparedness
A common strategy focusing on global priorities
Political commitment
Financial investment
International coordination
I’m sure you can see how most of these tie in with the WHA above. But the document is more detailed in regards to surveillance & data management -
Enhanced disease surveillance
Standardised methods
Integrated surveillance
Shipment of isolates and specimen
Collect additional (surveillance) data
Identify geographical gaps
Integration with polio and other existing surveillance
Integration with existing WHO surveillance network
Samples, information, rapid tests, commercial testing, clinical samples - all should be integrated
Regional/global meetings to ‘spread message’
Integrate with WOAH’s animal influenza surveillance
Database integration
Data harmonisation
Improve dissemination of existing records
Central database, should record epidemiological, virological, and genetic information
Common database records, case definitions
The next part relates to the analysis of the data above and drive the vaccine message -
Influence developing world through cost analysis to implement agenda
To ‘justify vaccine programmes’ and prioritise
To advance and drive vaccination targets
To provice vaccination coverage feedback to the central database
Then there’s the matter of political action and messaging -
To increase political subscription to common agenda
To drive a WHA item (which became the above)
For the WHO to create a ‘model plan’ (acknowledges the 1999 WHO Pandemic Plan, which was written by the ESWI)
The countries should perform self-assessment
Increased manufacturing capacity throughout the world, ‘equity of supply’, and other topics covered by WHA56.19 above
Evaluation of community control strategies
I will deal with the latter two first, and reserve more time for the former.
Political messaging - in short - means that the WHO will author a pandemic treaty, the nations should adopt said and identify where their implementation falls short. They even have a function to perform said evaluation - the Joint External Evaluation - but let’s set that aside for the time being.
The analysis of the data feeds even more information back into the central, global database - vaccination uptake - which will progressively be pushed in only one direction, until everyone is ‘vaccinated’, all the time. As part of this drive, the global database will also be used for economic analysis, to justify the global surveillance agenda in nations yet to commit.
The core message is one of surveillance, or rather - ‘enhanced disease surveillance’. What’s of importance is that it will be standardised, integrated, harmonised, central, and be expanded into geographical territories where it does not presently exist, or, in list form -
Standardised
All surveillance data should consistent and compatible. It’s no good comparing two distinct populations, if those are recorded in wildly different ways, with no immediate way to bridge the differences.Integrated
Surveillance data on influenza should be merged with polio surveillance data, other existing WHO networks, animal networks through WOAH’s animal influenza data (bridging the zoonotics), and all samples, rapid tests, commercial tests, and clinical samples further be included in the massive dataset.
Oh wait, what happened to all those covid tests?Harmonised
All data - including existing records - should be made to conform to uniform standards. This somewhat ties in with the standardisation above, but also affects existing records, and ultimately leads to the next point.Centralised
A single, central database (at the WHO) should contain all data gathered on everyone (including animals), and further contain epidemiological, virological, and genetic information.
The reason why the central database will be under the control of the WHO ties in with their next narrative - the health digital twin, which is outside the scope of this article.Geographically expanded
Those nations not yet subscribed, should be convinced through regional meeting peer pressure, or probably outright bribery.
Has it clicked yet?
-
What the two documents combined detail is global surveillance, with the express purpose of delivering vaccines to humans (and the other animals) to control disease. Or allegations thereof, anyway.
Wait, I recall something quite similar stated in the Manhattan Principles - aka One Health.
And while on the topic, let’s revisit principle 8 -
‘Restrict the mass culling of free-ranging wildlife species for disease control to situations where there is a multidisciplinar, international scientific consensus that a wildlife population poses an urgent, significant threat to human health, food security, or wildlife health more broadly‘
How do you interpret ‘more broadly’ in this context?
One Health: The Berlin and Manhattan Principles

In 2004, The Manhattan Principles were released. These are, in short, the 12 rules making up ‘One Health’. They go as per below - I’ve spent a fair amount of time trying to decipher their legit meaning. In general, some concepts encapsulate a number of these components; One Health is the ecosystem, which is what all life live within; humans, domestic ani…
-
Finally, let’s fit these two in chronologically.
1992
The ESWI (big pharma lobby group) launches in November
The first EU resolution arrives on the topic of disease control for sakes of human health - also in November1996
Claims of CJD through BSE leds to the culling of cattle to the tune of 1 million in the UK.1997
The absolutely fake zoonotic ‘pandemic potential’ H5N1 reaches Hong Kong. Future WHO General-Secretary Margaret Chan culls 1.6m chicken, thereby setting ‘pandemic’ precedent on the thinnest level of evidence recorded in human history. ESWI is involved through Ab Osterhaus, whose Dutch team arrives at the H5N1 conclusion.2003
The no-autopsy disagnosis-of-exclusion SARS allegedly runs rampant in Hong Kong, prompting the EU and the Hong Kong authorities to setup disease control centres, which immediately push for surveillance.2004
The Manhattan Principles - aka One Health - is born, outlining surveillance and vaccines, and include animals in this ‘approach’.
There were other, generally minor episodes here. But we are to believe that this all just fortuitously happened at a time, where political will was clearly prompting legislative action taken in one direction only? Uh yeah, another miraculous coincidence in my book.
The latter document - the World Health Assembly resolution - was released in 2003. Same year that saw the launch of PEPFAR. And that’s no coincidence, as surveillance was rolled out under that guise. More on that in a later article.
-
But I’ve reserved one thing for last. Because I know what you’re thinking - this happened immediately after 9/11, and consequently, bio/surveillance was a hot topic, also considering the hugely infringing Patriot Act, enabling the surveillance state in the United States - and never mind this legislation being drafted, debated, re-drafted, checked, and then headed for another couple of rounds of debate in the house and senate in a ludicrous 6 weeks only. Let’s set that aside. Let’s instead zoom in on a detail in the 2002 document, specifically -
‘Recognising the importance of further developing the capacity for influenza surveillance and control and for encouraging wider input and participation, the WHO Global influenza programme called for contributions to develop a Global Agenda in July 2001‘.
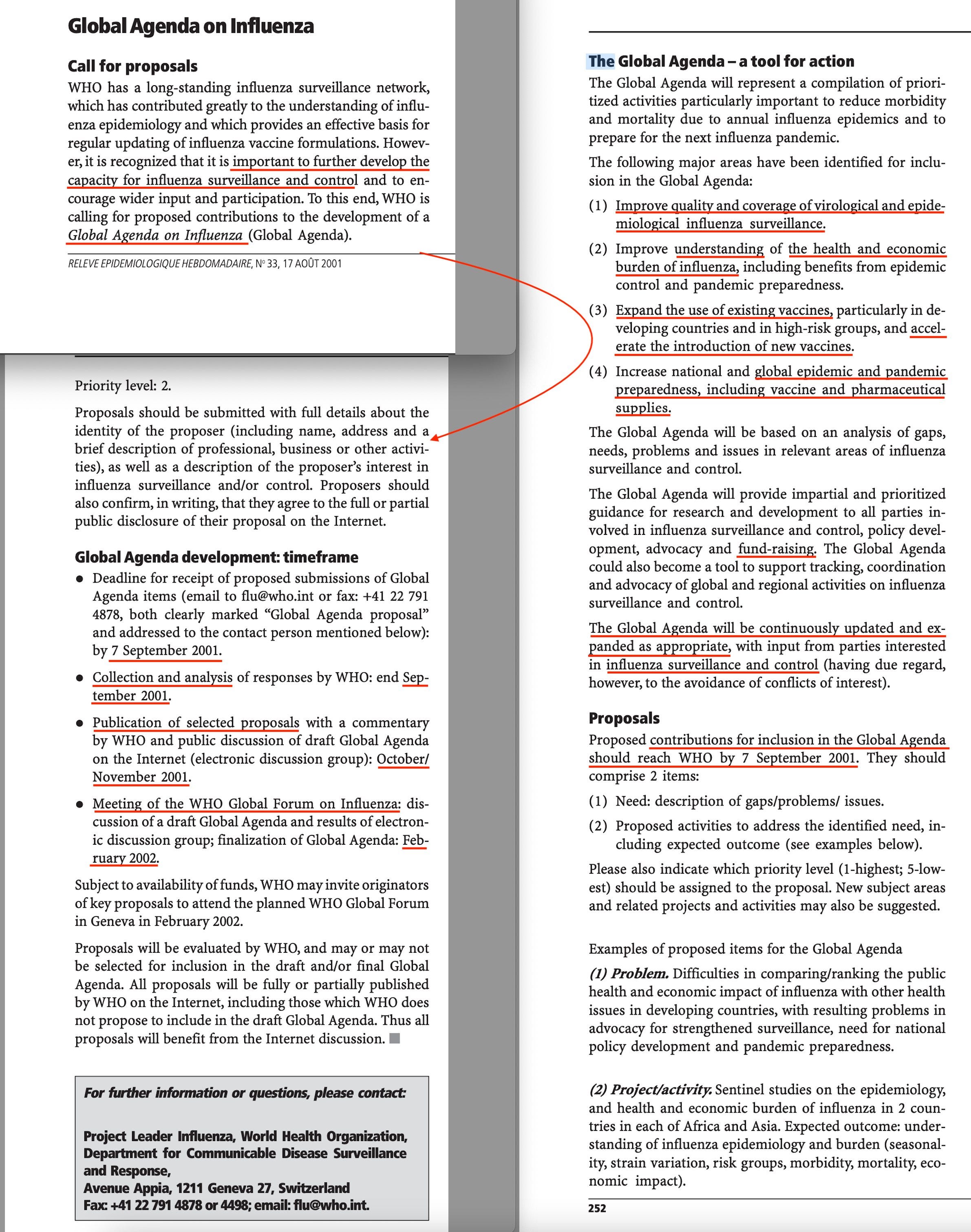
The call for contributions in other words was kicked off in July, 2001. But when was deadline for contributions?
Now, I don’t know if you’ll be able to see this link, but I can otherwise supply the PDF. I absolutely guarantee it’s a legit document. And the document outlines more on the process itself - and deadlines. And in that regard, from the link -
‘Deadline for receipt of proposed submissions of Global Agenda items (email to flu@who.int or fax: +41 22 791 4878, both clearly marked "Global Agenda proposal" and addressed to the contact person mentioned below): by 7 September 2001.’
Do you get it?
The proposal deadline arrived 4 days prior to 9/11.
Surveillance was on the agenda before those planes hit the towers.
-
The BSE episode is recorded via Wikipedia.

-
Here’s why I state that the 1997 H5N1 episode was manufactured horse manure.
The 1997 H5N1 Pandemic That Wasn't

Let's rewind to Hong Kong in the year 1997. Supposedly, when H5N1 left its terrifying mark, jumping from animal to human. The zoonotic event, which paved the ground for future action on what would eventually become One Health. Because this story... smells
-
Here’s my 3-part write-up of One Health.
One Health - Part 1: 1992 - 2020

Bringing One Health to Covid-19. - I grew up in Denmark, and thus, the mere mention of the year 1992 brings back fond memories of sitting 3 inches off the television, and going to the pub a with friends, where we drank to excess and watched football.